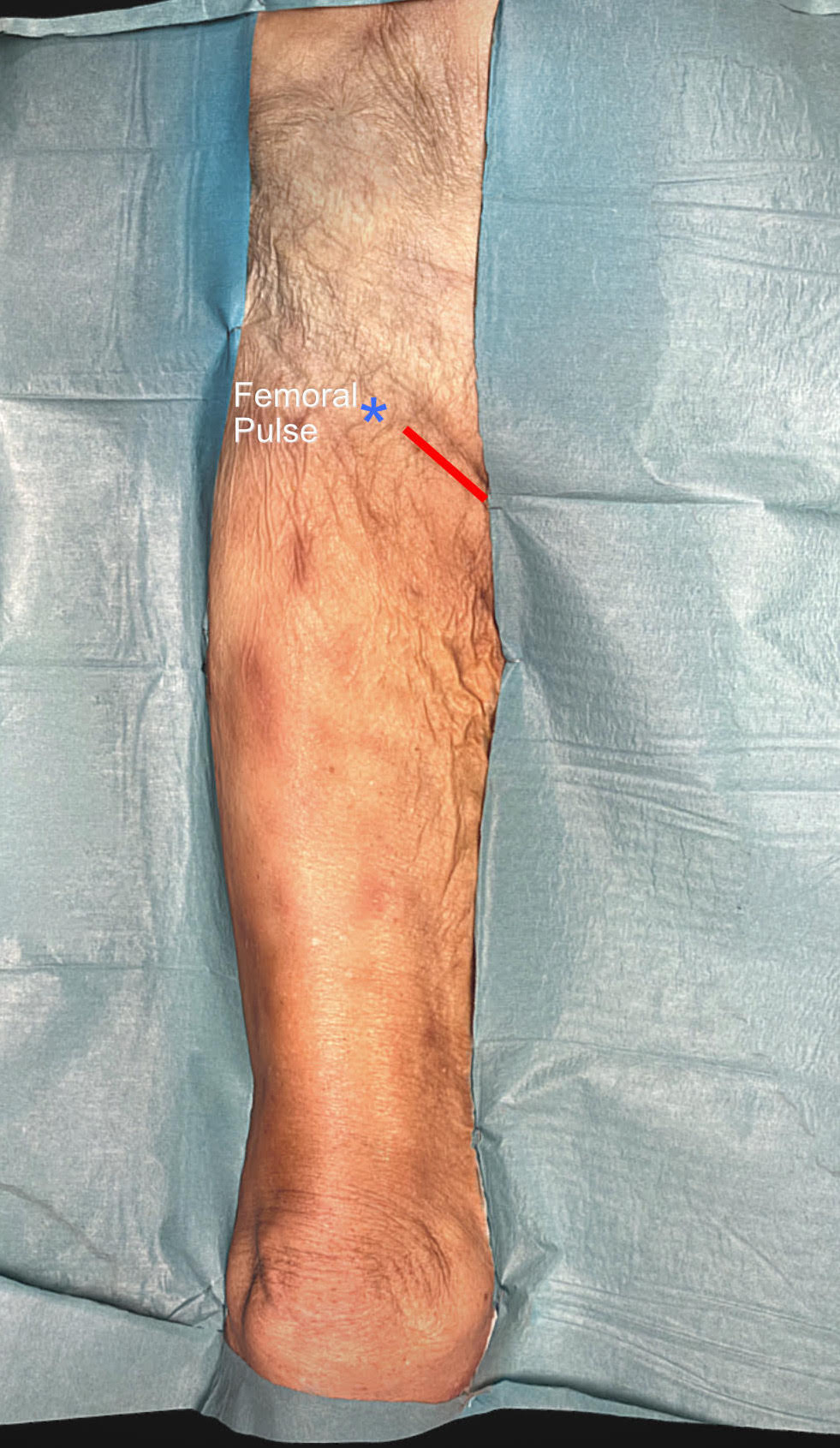
Skin incision: Patient supine with slight external rotation of the leg, foot 45 degrees. To mark the incision, palpate the pulse of the femoral artery and start the incision 3-4 cm medial to this and continue medially in the inguinal crease about 5-6 cm.
1. Pectineus m. and saphenous v
Incise the skin. In the subcutis you will find minor veins and small terminal cutaneous nerve branches from the ilioinguinal nerve, some of which can be spared. Define the superficial fascia, lift it up and divide, to find the saphenous vein at the lateral aspect of the incision, where it courses lateral towards the femoral vein. Hold it lateral, always stay medial to the vein.
Incise the skin. In the subcutis you will find minor veins and small terminal cutaneous nerve branches from the ilioinguinal nerve, some of which can be spared. Define the superficial fascia, lift it up and divide, to find the saphenous vein at the lateral aspect of the incision, where it courses lateral towards the femoral vein. Hold it lateral, always stay medial to the vein.
2. Obturator nerve exposed
Extra-pelvic approach to decompression of the obturator nerve
Instruments: Scalpel with blade 10, toothed forceps, small and large (articulated), and short Mayo-Adams self-retaining retractors, 5x1 cm Langenbeck retractor, scissors, artery clip, blunt dissector, bipolar forceps, needle holder. You may also use nerve stimulator.
Patient supine with slight external rotation of the leg, foot 45 degrees. To mark the incision, palpate the pulse of the femoral artery and start the incision 3-4 cm medial to this and continue medially in the inguinal crease about 5-6 cm.
Instruments: Scalpel with blade 10, toothed forceps, small and large (articulated), and short Mayo-Adams self-retaining retractors, 5x1 cm Langenbeck retractor, scissors, artery clip, blunt dissector, bipolar forceps, needle holder. You may also use nerve stimulator.
Patient supine with slight external rotation of the leg, foot 45 degrees. To mark the incision, palpate the pulse of the femoral artery and start the incision 3-4 cm medial to this and continue medially in the inguinal crease about 5-6 cm.
Remove the pubic hair and prep the area along the medial aspect of the inguinal crease, drape in the usual fashion.
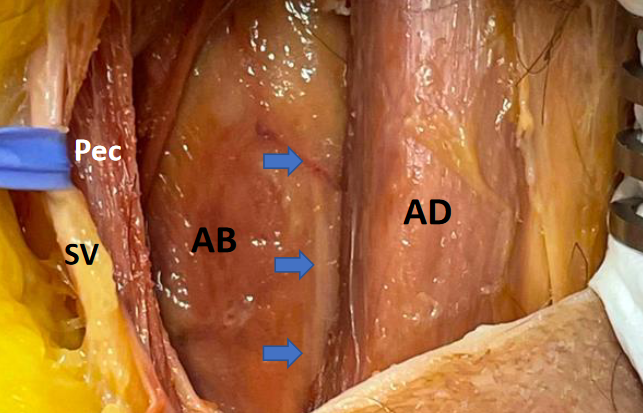
Incise the skin. In the subcutis you will find minor veins and small terminal cutaneous nerve branches from the ilioinguinal nerve, some of which can be spared. Define the superficial fascia, lift it up and divide, to find the saphenous vein (SV) at the lateral aspect of the incision, where it courses lateral towards the femoral vein. Hold it lateral, always stay medial to the vein. There is now additional fascia covering the transition between the pectineus muscle (Pec) laterally, and the adductor longus muscle (AD) medially. Open this fascia gently and identify the medial border of the pectineus. Run your finger up and down till it gradually develops a space between the pectineus and adductor longus and follow that space to the fascia and fat plane on the adductor brevis muscle (AB). You will now spot the obturator nerve (blue arrows) with accompanying vessels, embedded in fat and the neurovascular sheath.
Incise the skin. In the subcutis you will find minor veins and small terminal cutaneous nerve branches from the ilioinguinal nerve, some of which can be spared. Define the superficial fascia, lift it up and divide, to find the saphenous vein (SV) at the lateral aspect of the incision, where it courses lateral towards the femoral vein. Hold it lateral, always stay medial to the vein. There is now additional fascia covering the transition between the pectineus muscle (Pec) laterally, and the adductor longus muscle (AD) medially. Open this fascia gently and identify the medial border of the pectineus. Run your finger up and down till it gradually develops a space between the pectineus and adductor longus and follow that space to the fascia and fat plane on the adductor brevis muscle (AB). You will now spot the obturator nerve (blue arrows) with accompanying vessels, embedded in fat and the neurovascular sheath.
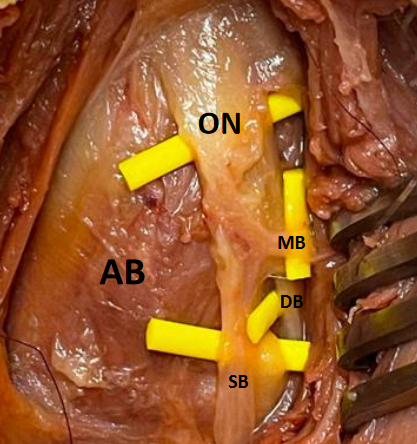
When you open the overlying fascia, you will find the motor branches (MB/DB)) for the adductor longus (AD) and the superficial branch (SB), which will end in the cutaneus branch, after supplying the brevis.
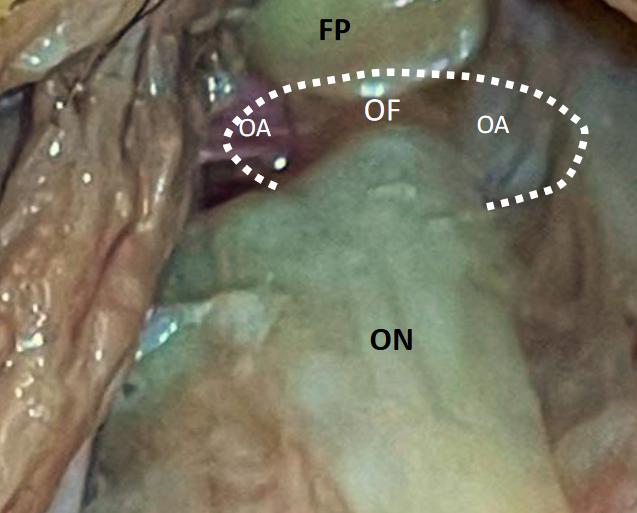
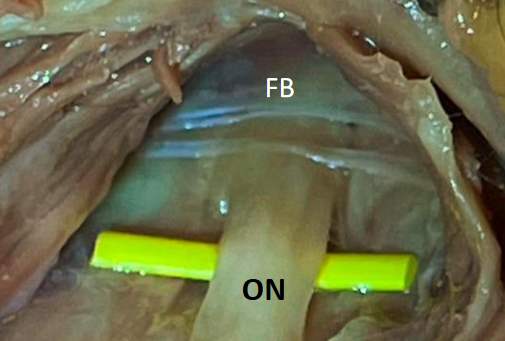
At this stage you can dissect the nerve proximally, all the way to the obturator foramen (OF), and identify any compression elements, which may be fascia bands (FB).
Be aware that the obturator arteries (OE) accompany the nerve in the foramen (here also covered by a fat pad (FP)), and avoid transecting them, as stopping hemorrhage here may well lesion the nerve directly, or by heat from the bipolar. With a thin blunt dissector, explore the foramen and make sure there is space. The most likely place of compression is the fascial bands crossing the nerve distal to the foramen.